Best Peptides for Fat Loss: Top 5 Research-Backed Options

Best Peptides for Fat Loss: Top 5 Research-Backed Options
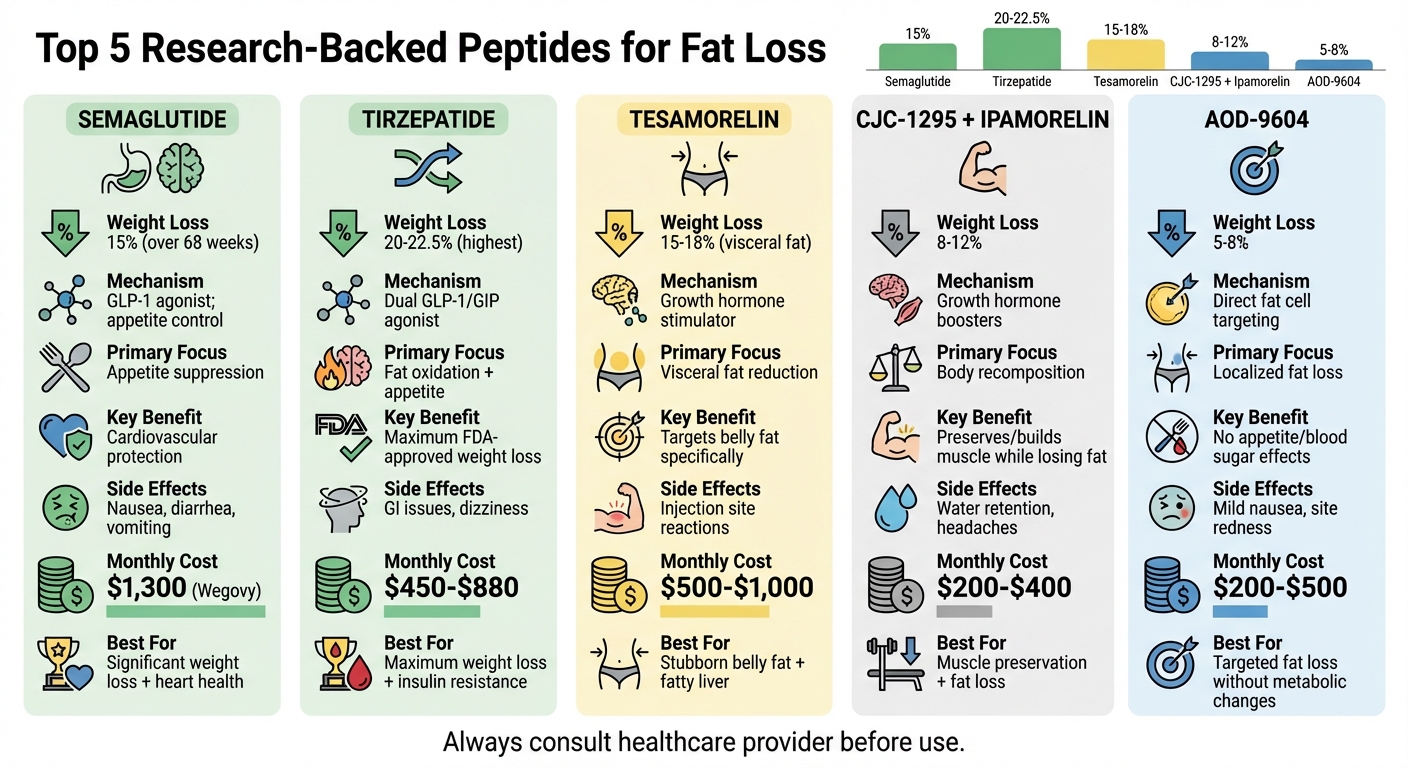
Peptides are becoming a popular tool for fat loss by targeting metabolism, appetite, and fat breakdown. The top five peptides for weight loss, supported by research, include:
- Semaglutide: FDA-approved GLP-1 agonist that reduces appetite and slows digestion. Clinical trials show up to 15% body weight reduction over 68 weeks.
- Tirzepatide: A dual GLP-1/GIP agonist offering up to 20-22.5% weight loss, surpassing Semaglutide in trials.
- Tesamorelin: Focuses on visceral fat reduction, particularly effective for belly fat and fatty liver disease.
- CJC-1295 + Ipamorelin: Boosts growth hormone levels, promoting fat loss while preserving muscle mass.
- AOD-9604: Targets fat cells directly without affecting appetite or blood sugar, ideal for localized fat reduction.
Each peptide has unique benefits, mechanisms, and safety considerations. For example, Semaglutide and Tirzepatide excel in overall weight loss, while Tesamorelin and AOD-9604 focus on specific fat types. Always consult a healthcare provider for proper use and monitoring.
Quick Comparison
| Peptide | Mechanism | Weight Loss (%) | Primary Focus | Common Side Effects | Cost (Monthly) |
|---|---|---|---|---|---|
| Semaglutide | GLP-1 agonist; appetite control | ~15% | Appetite suppression | Nausea, diarrhea, vomiting | $1,300 (Wegovy) |
| Tirzepatide | Dual GLP-1/GIP agonist | 20-22.5% | Fat oxidation, appetite | GI issues, dizziness | $450-$880 |
| Tesamorelin | Growth hormone stimulator | ~15-18% (visceral fat) | Visceral fat reduction | Injection site reactions | $500-$1,000 |
| CJC-1295 + Ipamorelin | Growth hormone boosters | 8-12% | Body recomposition | Water retention, headaches | ~$200-$400 (research-grade) |
| AOD-9604 | Direct fat cell targeting | 5-8% | Localized fat loss | Mild nausea, site redness | $200-$500 |
Peptides work best alongside proper nutrition, exercise, and medical oversight. Choose one that aligns with your goals and health needs.
Top 5 Peptides for Fat Loss: Comparison of Effectiveness, Mechanisms, and Side Effects
Doctor Explains Fat Loss Peptides - Best Stack for MAXIMUM Results!
1. Semaglutide
Semaglutide, a GLP-1 receptor agonist approved by the FDA, is marketed under two names: Wegovy (2.4 mg) for managing chronic weight and Ozempic for type 2 diabetes. It mimics the glucagon-like peptide-1 hormone, which plays a role in appetite control and food intake regulation.
How It Works
Semaglutide works on multiple fronts. It influences the hypothalamus to suppress appetite, slows gastric emptying to prolong feelings of fullness, and reduces the brain's reward response to food. Together, these effects help reduce calorie intake without causing intense hunger.
Research Highlights
The STEP 1 trial demonstrated semaglutide's effectiveness in weight loss. Among 1,961 participants with obesity, those taking 2.4 mg weekly lost an average of 14.9% of their body weight over 68 weeks. In contrast, the placebo group saw only a 2.4% reduction. Notably, 86% of those on semaglutide lost at least 5% of their body weight, and about one-third achieved a 20% or greater reduction.
The SELECT trial provided further evidence. Conducted with 17,604 adults who had cardiovascular disease and a BMI of 27 or higher (but no diabetes), the study found weekly semaglutide use led to a sustained 10.2% weight loss over 208 weeks. Additionally, participants experienced a 20% drop in major cardiovascular events and a 7.7 cm reduction in waist circumference.
"In SELECT, at 208 weeks, semaglutide produced clinically significant weight loss and improvements in anthropometric measurements versus placebo. Weight loss was sustained over 4 years." - Nature Medicine
These findings solidify semaglutide as a powerful tool for fat loss.
Advantages for Fat Loss
Semaglutide's benefits extend beyond shedding pounds. It also improves body composition. A 104-week study showed that 12% of participants achieved a healthy BMI (under 25 kg/m²), compared to just 1.2% in the placebo group.
Dosage and Guidelines
Semaglutide is administered as a once-weekly subcutaneous injection. To minimize gastrointestinal side effects, doses are gradually increased over 16–20 weeks. The recommended dosing schedule is:
| Dose | Duration | Phase |
|---|---|---|
| 0.25 mg/week | Weeks 1–4 | Initiation (non-therapeutic) |
| 0.5 mg/week | Weeks 5–8 | Early appetite suppression |
| 1.0 mg/week | Weeks 9–12 | Noticeable appetite reduction |
| 1.7 mg/week | Weeks 13–16 | Near-maintenance |
| 2.4 mg/week | Week 17+ | Full therapeutic maintenance |
For those using the oral version, Rybelsus, it should be taken on an empty stomach with no more than 4 ounces of water. Wait at least 30 minutes before eating or taking other medications [10, 16].
"Sufficient protein, in combination with regular physical activity, is crucial to minimize the loss of lean muscle while losing weight on Wegovy." - Dr. Lauren Lemieux, Obesity Medicine Specialist, FORM Health
The cost of Wegovy is about $1,300 per month without insurance, while compounded semaglutide is priced between $200 and $500 per month.
Safety and Side Effects
Gastrointestinal issues are the most common side effects. Approximately 44% of users report nausea, 30% experience diarrhea, 24% report vomiting, and constipation is also frequent. These symptoms are usually temporary and improve as the body adjusts to the medication.
Semaglutide carries an FDA boxed warning for thyroid C-cell tumors based on animal studies. It is not recommended for individuals with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 [10, 17]. Other potential risks include acute pancreatitis, gallbladder disease, and kidney injury, often linked to dehydration caused by gastrointestinal distress. There have also been reports of vision changes, including diabetic retinopathy complications and a possible increased risk of Nonarteritic Anterior Ischemic Optic Neuropathy (NAION).
Discontinuing semaglutide can lead to weight regain. The STEP 4 trial found that nearly two-thirds of lost weight returned within a year after stopping the medication. Women planning to conceive should stop semaglutide at least two months before pregnancy due to potential reproductive risks observed in animal studies. Additionally, its impact on gastric emptying raises the risk of pulmonary aspiration during surgery. A retrospective study noted a 6% increase in retained solid gastric contents during procedures.
2. Tirzepatide
After Semaglutide, another option making waves is Tirzepatide. Sold as Zepbound for weight management and Mounjaro for type 2 diabetes, it stands out as the first "twincretin", targeting both glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptors. This dual action sets it apart, offering a unique approach to fat loss.
Mechanism of Action
Tirzepatide works by reducing appetite through its effects on the area postrema and hypothalamus, leading to increased feelings of fullness and fewer cravings. It also slows down gastric emptying and enhances insulin sensitivity. By activating GIP receptors on fat cells, it promotes fat oxidation and significantly reduces both visceral and liver fat. These effects have been consistently supported by clinical studies.
Key Research Evidence
The SURMOUNT-1 trial involved 2,539 adults with obesity (but without diabetes). Participants receiving 15 mg of tirzepatide weekly saw an average weight reduction of 20.9% (around 48.5 lbs) over 72 weeks, compared to just 3.1% in the placebo group. In the 15 mg group, 91% of participants lost at least 5% of their body weight, compared to 35% in the placebo group. Another study, SURMOUNT-4, reported a total weight loss of 25.3% over 88 weeks.
Additional findings include a SURPASS-1 substudy, which showed a 26% reduction in total body fat mass, with fat loss outpacing lean mass loss by about three times. Meanwhile, the SURPASS-3 MRI substudy recorded an 8.1% absolute reduction in liver fat content from a baseline of 15.7%.
In direct comparisons with Semaglutide, tirzepatide consistently delivered greater weight loss. On average, participants achieved a 20% reduction in body weight with tirzepatide, compared to 14% with Semaglutide. Additionally, 82% of tirzepatide users lost at least 10% of their body weight, versus 61% for Semaglutide users.
Benefits for Fat Loss
Tirzepatide doesn't just reduce weight; it reshapes body composition. Visceral fat mass dropped by as much as 40.1%, and up to half of participants with type 2 diabetes achieved normoglycemia (HbA1c < 5.7%) at the highest dose.
Dosage and Administration
Tirzepatide is administered as a once-weekly subcutaneous injection, with a half-life of roughly five days. Treatment starts at 2.5 mg weekly for four weeks, increasing by 2.5 mg every four weeks until reaching a maintenance dose of 5 mg, 10 mg, or 15 mg. The monthly cost ranges from $450 to $880.
It's important to note that patients using oral hormonal contraceptives should switch to a non-oral method or add a barrier method for four weeks after starting or adjusting their tirzepatide dose due to possible drug interactions. Treatment should be stopped if a patient's BMI falls to 18.5 kg/m² or lower.
Safety Considerations
The most common side effects are gastrointestinal. At the 15 mg dose, nausea affects about 30% of users (compared to 10% with placebo), diarrhea occurs in up to 23%, and vomiting in up to 12%, with constipation also reported. These side effects are typically dose-dependent and most frequent during the dose-escalation period.
Tirzepatide is not recommended for individuals with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2. Additional side effects include alopecia (5% vs. 0.9% for placebo) and dizziness (4% vs. 2.3% for placebo). While serious adverse events are similar to placebo, higher doses may lead to increased discontinuation rates due to side effects. These findings highlight tirzepatide's potential as a research-backed option for weight and fat reduction.
3. Tesamorelin
Tesamorelin is a 44-amino-acid analogue of growth hormone-releasing hormone (GHRH), modified with trans-3-hexenoic acid to improve its stability. It was approved by the FDA in 2010 under the brand name Egrifta for the treatment of HIV-associated lipodystrophy.
Mechanism of Action
Tesamorelin works by binding to GHRH receptors in the anterior pituitary gland, prompting the release of growth hormone in a pulsatile manner. This process stimulates lipolysis, particularly in visceral adipose tissue, where fat cells have a higher density of growth hormone receptors.
"Tesamorelin does not add growth hormone to your system from the outside. Instead, it stimulates your own pituitary gland to release growth hormone in the same pulsatile pattern your body uses naturally." – PeptideFox
Unlike synthetic growth hormone (GH) injections, tesamorelin maintains the body's natural regulatory mechanism, known as the somatostatin brake. This prevents the extreme GH spikes that can occur with exogenous hormone use. Clinical studies have confirmed its ability to reduce visceral fat effectively.
Key Research Evidence
Phase III clinical trials, including LIPO-010 and CTR-1011, demonstrated that a daily 2 mg dose of tesamorelin reduced visceral adipose tissue (VAT) by 19.6% and 11.7% at 26 weeks compared to placebo. A 2023 study reported a 134% average increase in natural GH production with tesamorelin use. Another trial led by Harvard researchers found a 37% reduction in liver fat over 12 months and a 4.2 cm reduction in waist circumference within 12 weeks in patients with nonalcoholic fatty liver disease (NAFLD).
"The visceral-selective fat loss is the critical finding. Tesamorelin didn't just reduce overall body fat - it specifically targeted the visceral depot that drives metabolic disease." – The Peptide Guides
However, stopping treatment after 26 weeks led to a 24.5% regain of visceral fat by week 52, emphasizing the need for continued use to maintain results.
Benefits for Fat Loss
Tesamorelin stands out for its ability to target visceral fat while preserving lean muscle mass. Unlike GLP-1 agonists, which can result in 25–40% of weight loss coming from lean mass, tesamorelin helps retain up to 97.3% of lean muscle during periods of caloric restriction.
Dosage and Administration
The standard dosage for tesamorelin is a 2 mg subcutaneous injection once daily. The injection is typically administered in the abdomen, with rotation of injection sites to prevent irritation. For optimal results, it should be taken 30–60 minutes before bedtime and at least two hours after eating to align with the body's natural nocturnal GH pulses. Regular blood tests for IGF-1, fasting glucose, and HbA1c are advised due to GH's effects on insulin sensitivity. Research-grade tesamorelin costs around $79 per 10 mg vial, while pharmaceutical-grade Egrifta is priced at $500 to $1,000 per month.
Safety Considerations
Common side effects include redness at the injection site (9% vs. 3% for placebo), joint stiffness or pain (13% vs. 11%), muscle pain (6% vs. 2%), and fluid retention (5–10% vs. 1–6%). Clinical trials have reported injection site reactions in 30% to 51% of participants. For those experiencing itchy welts or histamine reactions, taking an H1 blocker like Cetirizine 30–60 minutes before the injection may help. Tesamorelin is contraindicated for individuals with active malignancies, as GH and IGF-1 can encourage cell proliferation. Additionally, it is banned by the World Anti-Doping Agency (WADA) for use in competitive sports.
sbb-itb-7fad836
4. CJC-1295 (Often Combined with Ipamorelin)
CJC-1295 is a synthetic analog of growth hormone–releasing hormone (GHRH) often paired with Ipamorelin to create a dual effect: steady growth hormone (GH) release combined with acute GH pulses. This combination supports fat breakdown and nutrient partitioning toward muscle tissue.
Mechanism of Action
CJC-1295 binds to GHRH receptors, increasing GH levels by 2- to 10-fold for over six days and boosting IGF-1 levels by 1.5- to 3-fold for 9–11 days. Meanwhile, Ipamorelin triggers quick GH pulses within 40 minutes of administration without significant effects on cortisol, prolactin, or appetite - even at doses up to 200 times higher than required for GH release.
"CJC-1295 essentially provides an extended-release platform for stimulating the GHRH receptor... creating a sustained 'background' signal for growth hormone production." – Peptide Unlock
These sustained hormone elevations promote fat loss while preserving lean muscle mass.
Key Research Evidence
Studies highlight the fat-reducing potential of GH secretagogues:
- In obese individuals, GH treatment reduced visceral fat by 35.3%, compared to 28.5% in the placebo group.
- Research on HIV-associated lipodystrophy showed a 42% reduction in visceral fat with high-dose GH, accelerating fat loss by 1.6 times compared to diet alone.
- GH-deficient adults experienced a 20% reduction in visceral fat after six months of GH supplementation.
Benefits for Fat Loss
The combination of CJC-1295 and Ipamorelin is particularly effective for reducing visceral fat while maintaining muscle mass. Unlike calorie-restricted diets that often result in muscle loss, this peptide stack preserves lean tissue. Additionally, Ipamorelin’s selectivity avoids hunger spikes and cortisol increases, common with older growth hormone–releasing peptides like GHRP-6.
Dosage and Administration
CJC-1295 is available in two forms:
- DAC (Drug Affinity Complex): Half-life of 6–8 days, typically dosed weekly.
- No DAC (Mod GRF 1-29): Half-life of about 30 minutes, requiring daily dosing.
The No DAC version is often preferred for fat loss protocols when paired with Ipamorelin. Here’s a sample dosing guide:
| Protocol Type | CJC-1295 (No DAC) Dosage | Ipamorelin Dosage | Frequency |
|---|---|---|---|
| Standard/Beginner | 100–150 mcg | 100–150 mcg | Once daily (before bed) |
| Advanced/Body Composition | 200–300 mcg | 200–300 mcg | 1–2 times daily (fasted state) |
| Maintenance | 100 mcg | 100 mcg | Once daily (bedtime) |
Subcutaneous injections are recommended in the abdomen, thighs, or glutes. For best results, administer on an empty stomach (2–3 hours after eating) and avoid food for 30–60 minutes post-injection, as insulin can interfere with GH pulses. Bedtime dosing aligns with natural GH surges during slow-wave sleep. A "5 days on, 2 days off" schedule helps maintain receptor sensitivity. Reconstitute with bacteriostatic water, inject slowly, and store the solution refrigerated (36–46°F) for up to 4–6 weeks.
Safety Considerations
Common side effects include mild injection site redness, water retention, and headaches. These peptides are not recommended for individuals with a history of cancer, as IGF-1 may promote cell growth, or for those with uncontrolled diabetes due to GH's potential to raise blood glucose levels. Regular monitoring of fasting glucose, HbA1c, and IGF-1 levels is advised, as prolonged GH elevation can affect insulin sensitivity. Most protocols suggest an 8–12 week cycle, followed by a 4–8 week break to allow the endocrine system to reset.
As of September 2024, the FDA removed CJC-1295 and Ipamorelin from the Category 2 bulk drug substances list. These peptides remain classified as research compounds and are not FDA-approved for therapeutic use.
5. AOD-9604
AOD-9604 is a synthetic peptide made up of 15 amino acids, derived from the C-terminal section (amino acids 177–191) of human growth hormone (hGH). Unlike other peptides that trigger growth hormone release, AOD-9604 works directly on fat cells, bypassing the pituitary gland and growth hormone receptors entirely.
Mechanism of Action
AOD-9604 acts as a beta-3 adrenergic receptor agonist in fat tissue, initiating a cAMP signaling cascade. This process activates hormone-sensitive lipase (HSL), which breaks down stored triglycerides into free fatty acids for energy use. Additionally, it inhibits enzymes responsible for creating new fat deposits, reducing the likelihood of future fat accumulation.
"The genius of AOD-9604 was in its conception: what if we could isolate just that tiny piece? Could we harness the metabolic power of hGH without triggering its other, sometimes undesirable, effects?" – Real Peptides
Importantly, AOD-9604 does not bind to growth hormone receptors or activate the IGF-1 axis. This means it supports fat loss without side effects like joint swelling, carpal tunnel syndrome, insulin resistance, or organ enlargement.
Key Research Evidence
Clinical studies back up these mechanisms, showing notable fat loss results:
- A 12-week randomized trial revealed that participants taking 1 mg/day lost an average of 2.6 kg (about 5.7 lbs), compared to 0.8 kg (about 1.8 lbs) in the placebo group.
- A Phase II trial in obese adults showed that 24 weeks of daily injections led to a loss of 3.8 kg (about 8.4 lbs) of abdominal fat, nearly triple the 1.3 kg (about 2.9 lbs) lost by the placebo group.
- A larger Phase 2b multicenter trial with 536 participants reported weight loss of 2.6% in the AOD-9604 group versus 2.3% in the placebo group, though this difference was not statistically significant.
- Preclinical studies in obese mice demonstrated a 28% reduction in body fat over just 19 days.
In practical use, individuals typically report losing 1–3 kg (about 2.2–6.6 lbs) during an 8–12 week cycle when paired with proper diet and exercise.
Benefits for Fat Loss
AOD-9604 targets fat directly without influencing appetite or blood sugar levels. Unlike GLP-1 agonists, which promote weight loss by suppressing appetite, this peptide focuses on breaking down fat metabolically. Evidence also suggests it may help preserve lean muscle mass during calorie restriction, and it avoids the anabolic or blood sugar-related effects of full-length growth hormone. Studies confirm that AOD-9604 does not affect insulin sensitivity or blood sugar levels.
Dosage and Administration
Standard doses range from 100 mcg to 300 mcg daily, administered via subcutaneous injection in areas like the abdomen, thigh, or upper arm. Rotating injection sites helps reduce irritation. Common dosing schedules include:
- Once daily: 200–300 mcg in the morning on an empty stomach
- Twice daily: 100–150 mcg in the morning and before workouts
- Frequency: 5–7 days per week, with 1–2 rest days to maintain receptor sensitivity
Cycles typically last 8–16 weeks, followed by a 2–4 week break. To ensure optimal absorption, administer the injection on an empty stomach and wait 30–60 minutes before eating.
The lyophilized powder should be reconstituted with bacteriostatic water using sterile techniques and stored in the refrigerator. Oral formulations are ineffective because peptides are broken down by stomach acid.
Safety Considerations
AOD-9604 is considered safer than full-length growth hormone. Side effects are generally mild and may include redness or swelling at the injection site, occasional headaches, nausea, or brief dizziness. Unlike hGH, it does not typically cause carpal tunnel syndrome, joint swelling, insulin resistance, or organ enlargement.
Currently, AOD-9604 is not FDA-approved in the U.S. and is available primarily as a research chemical. In Australia, it has been approved by the TGA under the brand name Aegerine for research use. However, it is banned by the World Anti-Doping Agency (WADA) under the S2.2 category (growth factors/peptides) for competitive athletes. Monthly costs for AOD-9604 typically range from $200 to $500, depending on the supplier and dosing protocol.
Comparison Table
The table below summarizes key findings from clinical studies on various peptides, providing a quick reference to help determine the best option for your fat loss goals.
| Peptide | Mechanism of Action | Proven Results | Primary Benefit | Common Side Effects | Best For |
|---|---|---|---|---|---|
| Semaglutide | GLP-1 receptor agonist; slows gastric emptying and signals satiety | Demonstrated weight loss efficacy over the medium term | Strong appetite suppression and cardiovascular protection | Nausea, vomiting, diarrhea, constipation | Those seeking significant weight loss with cardiovascular health concerns |
| Tirzepatide | Dual GLP-1/GIP receptor agonist; boosts fat oxidation and improves insulin sensitivity | Superior weight loss results over 72 weeks | Maximum FDA-approved weight loss potential | Nausea, diarrhea, decreased appetite, injection reactions | Individuals needing maximum weight loss or managing insulin resistance and Type 2 diabetes |
| Tesamorelin | GHRH analog; stimulates natural growth hormone release | ~15–18% reduction in visceral fat over 26 weeks | Targets dangerous visceral fat specifically | Injection site redness, joint pain, elevated IGF-1 | People focusing on reducing stubborn belly fat or addressing fatty liver disease |
| CJC-1295 + Ipamorelin | GHRH + GHRP synergy; amplifies growth hormone pulse frequency and magnitude | 8–12% weight loss with better body composition | Preserves/builds lean muscle while reducing fat | Water retention, flushing, increased hunger, head rush | Those prioritizing body recomposition over pure weight loss |
| AOD-9604 | GH fragment (177-191); promotes lipolysis and blocks lipogenesis | 5–8% weight loss | Encourages targeted fat reduction without appetite suppression | Injection site pain, headaches, mild nausea | Individuals aiming for fat loss without metabolic or appetite changes |
This breakdown emphasizes how each peptide offers distinct advantages, making it easier to align options with specific fat loss objectives.
For instance, Tirzepatide stands out for its unparalleled weight loss potential, achieving up to 22.5% weight loss compared to Semaglutide's 14.9%. Meanwhile, Tesamorelin is the only FDA-approved peptide explicitly designed to reduce visceral fat, a key concern for those with conditions like metabolic syndrome or fatty liver disease.
The CJC-1295 + Ipamorelin combination is ideal for individuals focused on body recomposition, helping to burn fat while preserving or increasing lean muscle mass. On the other hand, AOD-9604 provides a targeted approach to fat breakdown, making it a good choice for those who don't need appetite suppression or metabolic changes.
Conclusion
Peptides can significantly boost results when paired with solid lifestyle habits. As Kristi Sawicki explains:
"Peptides aren't shortcuts - they're amplifiers. The best results still come when your foundations are strong: strength training, protein intake, restorative sleep, and stress management."
Whether you're looking at Semaglutide with its 15% weight loss potential, Tirzepatide delivering reductions of 20–22.5%, or Tesamorelin targeting visceral fat, these compounds shine brightest when combined with proper nutrition, regular exercise, and sufficient sleep.
Medical oversight is non-negotiable when using these peptides. Avoid providers who skip essential evaluations like blood work or physical exams. Qualified healthcare professionals screen for risks (e.g., cancer history) and create personalized plans to prevent weight regain. Regular follow-ups are key to managing risks and sustaining results.
The quality of the peptide is just as important as the choice of compound. For FDA-approved options like Semaglutide or Tirzepatide, stick to licensed pharmacies or trusted telehealth services with prescribing physicians. If you're considering research-grade peptides, insist on third-party lab testing and batch-specific Certificates of Analysis showing purity levels of 98–99%. Be wary of prices that seem too good to be true - they often signal compromised or underdosed products.
While research is advancing toward multi-receptor agonists and mitochondrial enhancers, the advice from PeptideDeck remains timeless:
"The best peptide is one that matches your physiology, fits your lifestyle, and you'll use consistently. Superior protocols fail when adherence suffers."
Ultimately, the key is finding a peptide that aligns with your health goals, lifestyle, and ability to stay consistent. Instead of chasing the latest trend, focus on what works for you and your unique needs.
FAQs
Which peptide is best for belly fat vs overall weight loss?
Semaglutide and tirzepatide are recognized for their effectiveness in promoting overall weight loss, including reducing body fat. These medications work by regulating appetite and metabolism, making them powerful tools for weight management. When it comes to belly fat, specifically, GLP-1 receptor agonists like these are particularly helpful. They contribute to lowering visceral fat by enhancing metabolic health. Clinical studies strongly back the use of both peptides for these purposes.
How do I choose between Semaglutide and Tirzepatide?
Deciding between Semaglutide and Tirzepatide comes down to your personal health goals and how your body reacts to each medication.
- Semaglutide works well for controlling appetite. If curbing cravings is your main priority, this might be the better choice.
- Tirzepatide targets both GLP-1 and GIP receptors, and studies suggest it delivers more significant fat-loss results overall. If your goal is maximum weight reduction, this could be the way to go.
The best option varies from person to person, so it's important to consult with a healthcare provider. They can help you weigh the benefits and decide which medication aligns best with your needs.
What labs should I monitor while using fat-loss peptides?
Monitoring your health is crucial when using fat-loss peptides. Pay close attention to blood sugar levels, liver and kidney function, cholesterol levels, and overall metabolic health. Peptide therapies can affect these areas, so regular testing ensures both safety and effectiveness throughout the process.